
One of the most common running injuries we treat in our clinic is shin splints or Medial Tibial Stress Syndrome (MTSS). Shin splints cause one in five athletes to stop running. In addition to running, engaging in soccer, rugby, basketball, volleyball, or any sport that involves running or jumping can cause shin splints.
Symptoms
Most people would describe the initial pain of shin splints as a dull ache along the inside of the the lower leg (tibia). Shin splint pain is often felt at the beginning of a run and then diminishes as the run continues, only to return near the end of the run. In this initial stage the pain from shin splints will often dissipate completely with rest. If the shin splints progress, the pain will often be present with both activity and rest. Once shin splints reach the stage of constant pain, a medical professional should be seen to determine if additional injuries are present (stress fractures or compression syndrome).
The exact location of shin splints is often hard to find, because it is usually more of a diffused pain in the soft tissue (fascia, tendon, muscle) rather than on the bone (tibia) itself.
Causes of Shin Splints
The most common cause of shin splints is repetitive motion. This is not surprising considering the force of impact of each runner’s stride. A runner’s shins are subject to two to three times the runner’s body weight on foot impact. This high level of force can easily overwhelm the shin muscles (dorsi flexors) if they are not strong.
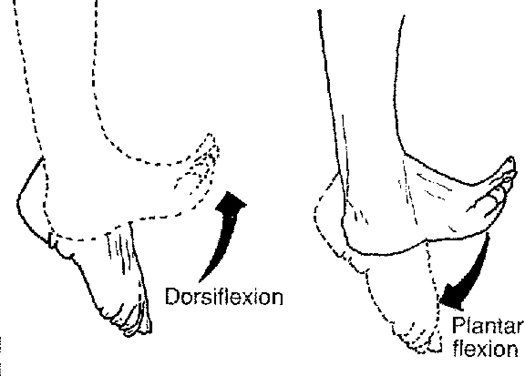
Shin muscles are called dorsi flexors because of the motion they perform with contraction. On contraction the dorsi flexors pull the foot up towards your shins, this is what is referred to as dorsi flexion. During running, the dorsi flexor muscles also control plantar flexion, through the process of eccentric contraction. Eccentric contraction occurs when a muscle elongates while under tension. Controlling plantar flexion of the foot is not an exclusively linear motion. As the foot strikes the ground it is subjected to both rotational forces (pronation and supination) and side to side motions.
{kind=link}
Any type of muscle imbalance, or abnormal motion pattern in the ankle, knee or hip could cause increased stress on the dorsi flexors as they try to control motion. In other words, the dorsi flexorsmay be the site of the shin splints, but the root cause could be far from the location of symptoms. For example, we know that excessive pronation (flat feet) will increase the load placed on thedorsi flexors as they try to control plantar flexion. We also know that weak or imbalanced external hip rotators (gluteus muscles) will increase pronation of the foot. Though it may not be a direct connection, weak external hip rotators could be part of the development and continuation of shin splints.
When it comes to shin splints, it is important to address the problems in all potential problem areas as well as the symptomatic structures in order to identify the root cause of the problem.
Differential Diagnosis
It is very important in diagnosing shin splints to make sure that you are actually dealing with shin splints and not a stress fracture or a case of compartment syndrome.
Stress Fractures
See our recent blog on Stress Fractures to review this condition.
Compartment Syndrome
Another condition that must be ruled out is compartment syndrome (CS). The muscles of our legs are divided into rigid compartments. These compartments are bound by strong fibrous tissue (deep fascia), and bones.
The anterior compartment contains some very important structures. It contains the dorsi flexors, the muscles directly linked to shin splints.
Anterior compartment Contains:
· Dorsiflexion muscles of the ankle and foot
CS occurs when the pressure inside these compartments increases to the point where it interferes with the blood supply to your muscles and nerves. This can occur when the muscle inside the compartment becomes too large, increasing the pressure. CS can also occur from trauma, bleeding, swelling, overuse or even excessive medication.
In a case of anterior compartment syndrome, a runner may experience sharp pain and swelling over the shins. They may also notice weakness of the dorsi flexors, especially against resistance. In addition there is often a decrease in the extremities pulse and a decrease in sensation. There are two types of compartment syndromes: chronic and acute.
Chronic Compartment Syndrome is not a medical emergency and can often be treated with manual therapies (ART, Graston, Massage). Chronic CS is also referred to as exertional CS. The pain of exertional CS in runners usually comes on with the first 15 minutes of running, then subsides within an hour after the run. The pressure of these compartments can be measured by a medical practitioner. A resting pressure of greater than or equal to 15 mm Hg is an indication that compartment syndrome is present.
Acute Compartment Syndrome could be a serious limb-threatening condition. Any delay in treatment may lead to infection, complications and even limb amputation. In most cases an acute compartment syndrome occurs after a traumatic event, and is most commonly seen with traumatic fractures.
If you suspect a stress fracture or compartment syndrome you need the help of a medicial practitioner.
Manual Therapy
Any type of restriction that forms in the dorsi flexors, or other related areas should be removed for a full resolution of shin splints. Some of these restrictions can be removed through the process of self-myofascial release (foam rollers, and stretching). If the restrictions are severe, a manual therapy practitioner (ART, Graston, Fascial Manipulation, Massage) will be needed to break the restrictions.
- The TA dorsiflexes and inverts the foot. In running, the TA is twice as active as many of the other muscles in the lower extremity. Consequently it is easily fatigued if weak. Once fatigue sets in, abnormal pronation is likely to increase.
- The EDL dorsiflexes the foot.
- The Peroneus Tertius is weak dorsiflexion of the ankle joint and is used to evert the foot at the ankle joint.
- Stand with your back to the wall, have your feet about 12-18 inches away from the wall.
- Lean back against a wall with your shoulders and gluteus touching the wall.
- Keep your heels on the ground, dorsi flex both ankles at the same time to maximum dorsiflexion. Then slowly lower your feet to almost touching the ground and repeat immediately.
- Do 10 to 15 repetitions then walk around for a short time. Do a total of 2 to 5 sets, depending on the strength of your dorsiflexors.
- Repeat this exercise every other day. Once you have done this exercise for several weeks, combine this exercise with version two.
- With your feet straight ahead walk on your heels (maximum dorsi flexion) with short steps for about 15 – 25 meters, depending on your strength. Your legs should be straight, but your knees should not be hyper extended.
- Next do exactly the same procedure, but this time with your feet turned outward.
- Finally perform the same procedure with your feet turned inward.
- Note: This exercise can also be performed on your toes.
A runner at this level recycles about half their energy through elastic recoil. This process is very similar to a spring mechanism, loading and releasing the spring with each stride. Part of this amazing spring mechanism is the dorsi flexor muscles.
Treatment of Shin Splints (MTSS)
The classic treatment of shins splints involves: rest, icing, elevation, compression and some easy stretches. This is good advice especially in the acute stage of the injury. However, exclusively following this advice will not prevent the return of the problem.
In order to resolve MTSS, the removal of any myofasial restrictions that may have formed in the soft tissue is required. This will be done in combination with a program of functional strengthening exercises for both the dorsi flexors and other areas that are affecting gait stability.
Any time a restriction is removed from one muscle the antagonistic and synergist muscles must also be assessed for restrictions. This is a key point that many manual therapists fail to recognize. For a full resolution, myofascial adhesions must be removed from the entire kinetic chain.
The following list of dorsi flexor muscles are common sites of adhesion removal, but a much larger kinetic chain must also be assessed and treated if necessary.
Dorsi Flexors (Primary)
Exercise
As with all musculoskeletal conditions, exercise is essential for a full resolution. Just because passive therapy has eliminated the symptoms does not mean the condition will not return. The following exercises are example of exercises that we prescribe to our patients with shin splints.
Strengthening Exercise – Example
Shin Raises – This is a great exercise for strengthening the dorsi flexors. It is best not to overdue this exercise at first, give your dorsi flexors time to adapt to the exercise. Slowly increase to the recommended number of repetitions and sets.
Version Two: This exercise is similar to version one except in two important aspects. First, the repetitions are performed at a much faster rate. Second the range of motion in which the exercise is performed is reduced.
Stretching Exercises - Example
Dynamic Shin Stretch – This dynamic stretches should be performed after a short warm-up.They are great for developing shin strength and overall motion control.
Heel Walking
There are numerous strengthening and dynamic stretching exercises that we recommend to our patients for the prevention and treatment of shin splints. The exact exercises that we recommend will vary depending on which areas of the patient’s kinetic chain are weak or restricted. In prescribing exercises, it is very common to prescribe both core and hip exercises as well as the exercises that directly affect the muscles of the shins.
If you would like information about our clinic in Calgary Alberta please go to www.kinetichealth.ca.
(COPYRIGHT KINETIC HEALTH 2012 – ALL RIGHTS RESERVED)
(COPYRIGHT KINETIC HEALTH 2012 – ALL RIGHTS RESERVED)
Greetings ! Medical Coding and certification has good demand. Don't miss the Opportunity. Coding System has changed everything, industry needs skilled coders.
ReplyDeleteCPC Certification Training