
An ankle sprain refers to the tearing of the ligaments of the ankle and account for approximately 40% of all athletic injuries. 85% of ankle sprains occur on the outside (lateral side) of the ankle and are known as an inversion sprain. This is the type of injury that most runners experience when they sprain their ankles. Medial ankle sprains (along the inside of the ankle) occur less frequently and are usually caused by fractures or other traumatic events.
So, why is an inversion sprain so common? You can put it down to our lopsided anatomy! The bone on the lower outside of the ankle (the lateral malleolus - distal fibula) extends further down than the bone on the inside of the ankle (medial malleolus – fibula). This difference gives the inside of the ankle (medial side) more stability than the outside of the ankle (lateral side).
At a symptomatic level, most ankle sprains appear to resolve completely without rehabilitation. In reality, ankle sprains that have not been rehabilitated correctly are usually susceptible to further injury.
Anatomy of an Ankle Sprain
The outside (lateral side) of the ankle achieves its stability from a three-ligament complex. These three ligaments are the:
In an inversion sprain, the Anterior Talofibular ligament (ATFL) is the most commonly injured. Ligaments in the ankle are named according to the bones to which they connect. In this case, the Anterior Talofibular ligament connects to the talus bone of the ankle as well as to a long bone of the lower leg - the fibula. The function of the ATFL is to prevent forward (anterior) displacement of the ankle (the talus).
In a severe ankle sprain another ligament called the calcaneofibular ligament (CFL) may also be damaged. This ligament connects your heel bone (calcaneous) with the fibula. This is a stronger ligament than the ATFL, and is not damaged as easily.
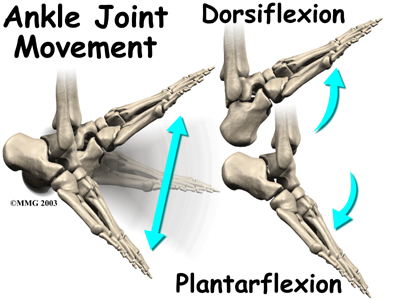
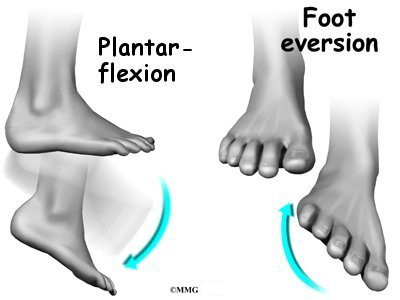
Both the ATFL and the CFL are usually damaged in motions where the foot is both pointed down (plantar flexed) and rolled out (inverted). Considerable instability in the ankle can occur when both these ligaments are injured.
{kind=link}
{kind=link}
The posterior talofibular ligament (PTFL) is not injured very often, except when there is a complete dislocation of the ankle (talus). The PTFL is the strongest ligament in the lateral complex.
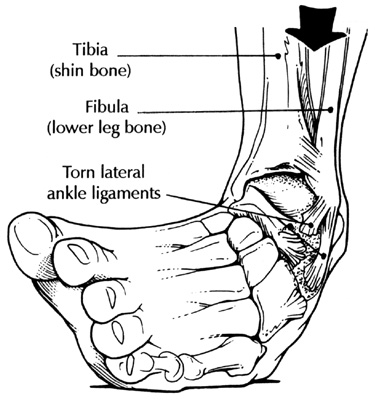
Another sprain injury that is becoming more prevalent is called a “High Ankle Sprain” (syndesmotic ligament complex). In this injury, the ligament and connective tissue between your shin bones (tibia and fibula) are torn. This is a serious injury that may require surgery to resolve.
{kind=link}
Not Just Ligaments
An ankle sprain may also result in damage to other structures. You may also experience damage to connective tissue, tendons, muscles further up the ankle, and even to the bones (possible fractures). This is why, with a severe ankle sprain, it is important to see a medical professional who can determine exactly which structures have been injured, and then provide treatment recommendations.
Treatment of Ankle Sprain
There are a number of things you can do to treat ankle injuries.
Just After The Injury
Immediately after spraining your ankle, it is important to do everything you can to reduce the swelling in the ankle. The faster you can implement treatment, the faster you will recover. An ankle sprain injury that is addressed quickly will often resolve in short period of time. If the injury is ignored, the ankle sprain could be prolonged for extensive periods of time.
So, immediately after the injury, while still in the acute stage - use RICE - rest, ice, compress, and elevate!
• R = Rest: During this stage, it may be necessary to take all weight off of the injured ankle. In such cases, crutches are commonly used. In my opinion, it is important to quickly return to weight-bearing as soon as possible to improve healing. I have found that reintroduction of weight-bearing stresses tends to decrease recovery time. When should you do this? As soon as possible, but not too soon! Rest is also essential.
• I = ICE : See our Blog about icing. Ice for at least 20 to 30, minutes 4 to 5 times per day to reduce swelling.
• C = Compression: Compression (with an ACE wrap) reduces both swelling and bleeding. With a Grade 3 sprain, wear a brace at all times until you are able to bear weight on your ankle.
{kind=link}
Once you have used “RICE”, it is very important to introduce motion into the ankle as soon as possible. Depending on the degree of injury, the patient could be asked to perform gentle ankle circles, or if able to do so, write the alphabet with their feet. Light calf stretching and using a stationary bicycle may also be beneficial.
If you are going to use medication (NASID’s) to reduce inflammation, be sure not to use them for more than seven days. Using anti-inflammatory medications for long periods of time inhibits tissue remodeling. See our Blog about Recommendations to Reduce Inflammation without Medication.
Manual Therapy for an Ankle Sprain
Manual therapy can make a huge difference in the recovery and prevention of an ankle sprain. By manual therapy, I am referring to techniques such as Active Release, Graston Technique, Massage Therapy, Fascial Manipulation, Manual Manipulation, and other manual procedures. In my opinion, these procedures are essential in the rehabilitation of an ankle sprain since they all act to break down and prevent scar tissue formation.
Manual therapy also speeds healing by increasing blood supply, oxygen, essential nutrients, and displace waste products that accumulate after an injury. This is especially important in treating ligaments because they generally have a very poor blood supply to begin with.
It is Important to Treat More Than Just the Ligaments
Earlier, I mentioned that there might be damage to several types of structures after an ankle sprain, especially the connective tissue, tendons, muscles, and nerves. The following is list of structures that are often injured in a lateral ankle sprain (inversion sprain).
{kind=link}
Ligaments
• Anterior talofibular ligament (ATFL) – Most common injured structure.
• Calcaneofibular ligament (CFL) – Second most commonly injured structure.
Tendons
o With an inversion sprain, it is common for the tendons of the peroneal muscles to be injured. It also common for the peroneal tendon to move out of its normal position (subluxate) during the recovery stage of an ankle sprain.
Muscles
• Peroneus brevis muscle – Longitudinal tears of the peroneus brevis are commonly associated with lateral ankle sprains.
• Peroneus longus muscle – These muscles often show a different activation pattern when there is ankle instability. This is often due to restrictions that have formed in the muscle. These restrictions, if not removed, could make a person more susceptible to future injuries.
Both muscles, evert the foot at the tarsal joint, and plantarflex the foot at the ankle.
{kind=link}
{kind=link}
Retinaculum
o During a lateral ankle sprain, the foot rolls inwards with considerable force. This forceful action can tear the peroneal retinaculum. This retinaculum is a band of connective tissue that keeps the peroneal tendons in place. When a tear in the retinaculum occurs, patients will notice a snapping sensation in the lateral ankle. Conservative treatment is 4 to 6 weeks in a short leg cast. However, a severe tear of the retinaculum is not a candidate for standard manual therapy and may require corrective surgery.
Nerves
• Superficial peroneal nerve - This nerve is at risk for traction injury during a lateral ankle sprain (inversion sprain).
If you would like information about our clinic in Calgary Alberta please go to www.kinetichealth.ca.
(COPYRIGHT KINETIC HEALTH 2012 – ALL RIGHTS RESERVED)
Serves as temporary treatment. But feels relieved.
ReplyDeletegout treatment